
CASE20220812_003
Simultaneous No-reflow Phenomenon and Abrupt Vessel Closure In Rotational Atherectomy Result in Cardiac Arrest.
By
Presenter
Wongwaris Aphijirawat
Authors
1
Affiliation
, Thailand1
Complications - Complications
Simultaneous No-reflow Phenomenon and Abrupt Vessel Closure In Rotational Atherectomy Result in Cardiac Arrest.
1
, Thailand1
Clinical Information
Patient initials or Identifier Number
Mr. LS
Relevant Clinical History and Physical Exam
Case 60 years old man with HT, DLP, ESRD on Regular H/DCC : Chest pain 10 hours PTA
PI : 10 hours PTA Patient reported substernal chest pain during hemodialysis at the last hour of session and the pain persisted for 40-45 mins.He also reported dyspnea and palpitation.PE : HR 90 bpm, BP 140/70 mmHg, RR 24 /minHeart : Normal S1, S2, no murmurLungs : minimal crepitation both
ECG showed Normal sinus rhythm with poor R wave progressionhstropt rising 73 to 210NSTEMI was diagnosed.
ECG showed Normal sinus rhythm with poor R wave progressionhstropt rising 73 to 210NSTEMI was diagnosed.
Relevant Test Results Prior to Catheterization
Echocardiogram : Concentric LVH, Borderline LV systolic function, LVEF 50-55% with anterior wall hypokinesia.No significant valvular pathology.
Relevant Catheterization Findings
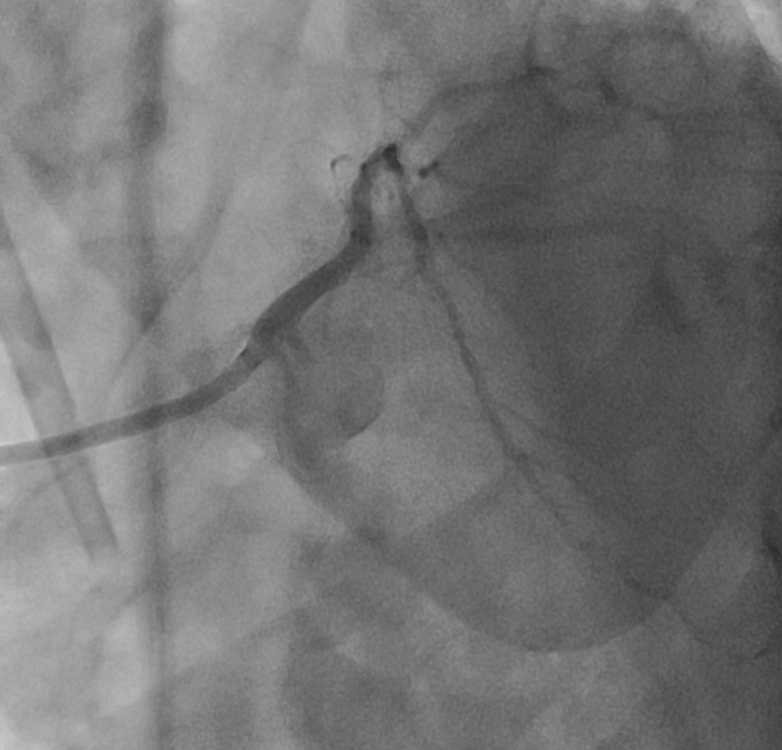
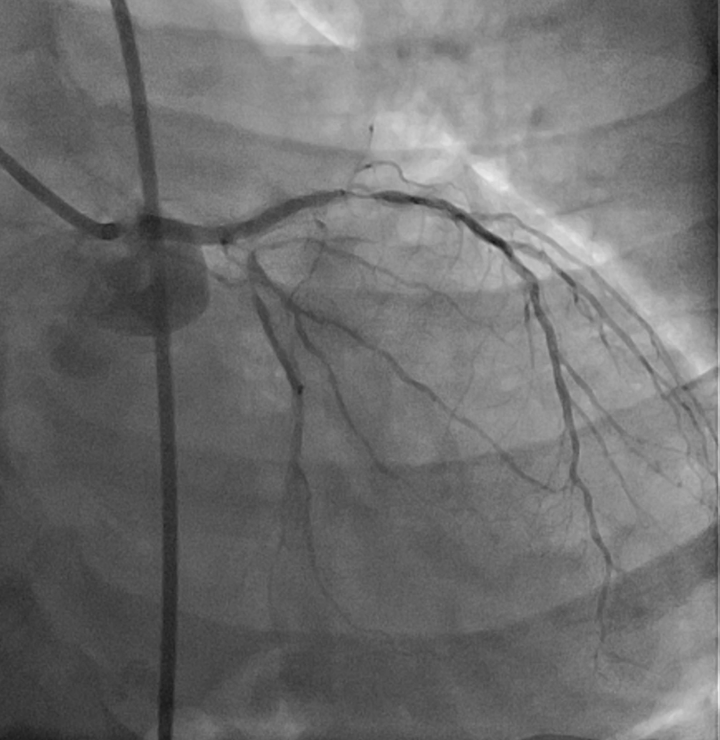
Left main : 50% stenosis at distal segment.LAD : 70% stenosis at proximal segment, 90% stenosis at mid segment, 80-90% stenosis at DG1. Severe calcified along vessel.Lcx : 90% stenosis at ostial - proximal segment.RCA : Dominant vessel with non-significant stenosis.

 Baseline angiogram.mov
Baseline angiogram.mov
IVUS LAD-LM.mp4
Interventional Management
Procedural Step
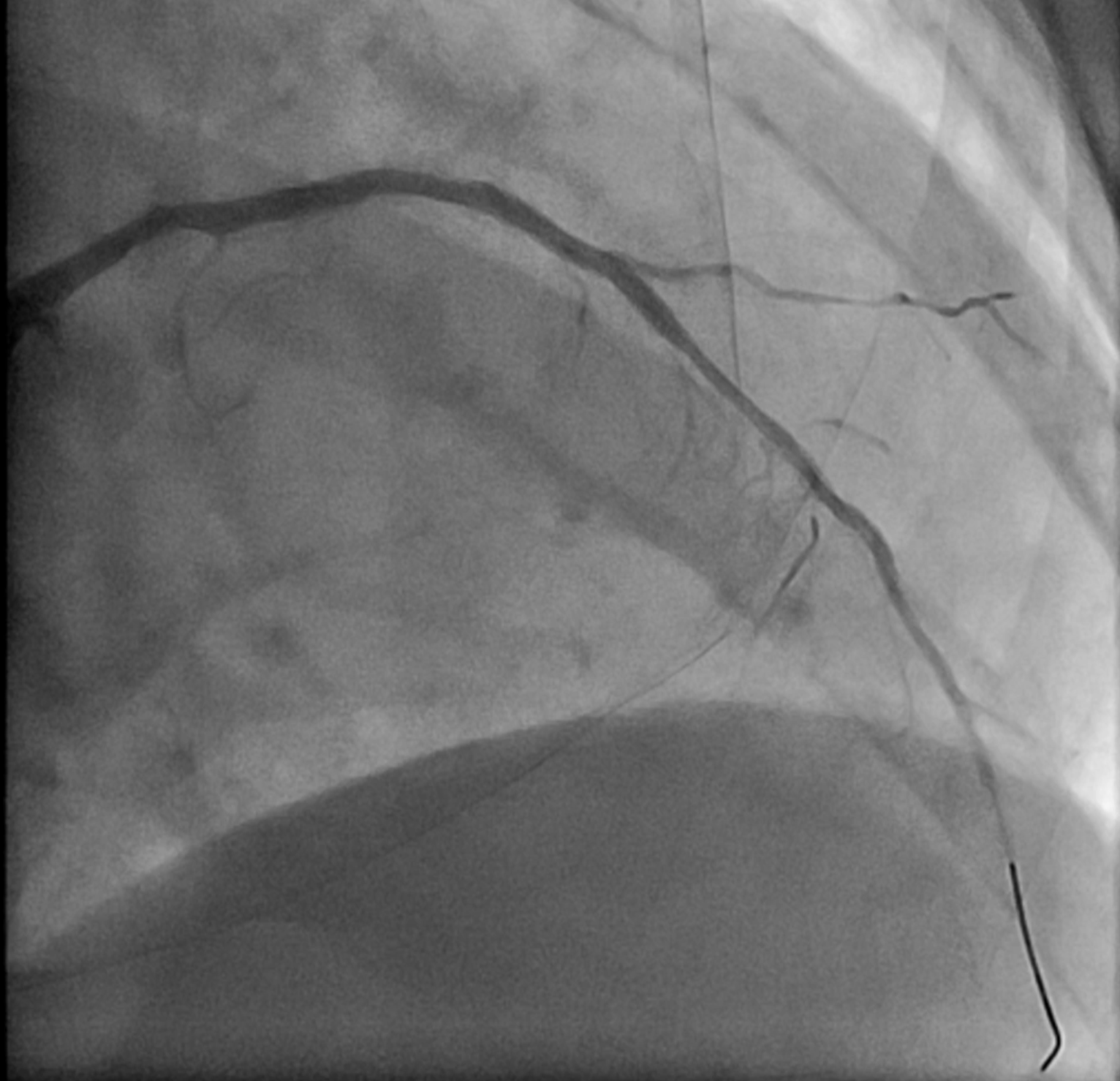
7F SL guiding catheter was engaged LCA. IVUS showed circumferential calcification at distal LM (MLA = 4.7 mm2) and mid LAD.1.5 burr Rotablator was runs at 200,000 RPM for 2 runs, 140,000 RPM for 3 runs with ease of rota burr pass to distal LAD.2.0 burr Rotablator was runs at 180,000 RPM for 3 runs. After rotaburr pass the lesion, patient developed chest pain and sudden hypotension -> cardiac arrest.CPR was started. Angiogram showed no-reflow phenomenon of LAD - Adrenaline IC ,aspiration thrombectomy was administratered due to emboli was suspected.However, No-reflow wasn't resolved after medication, CPR was continued. 2.5 x 15 mm SC balloon was dilated at distal-mid LAD - flow was restored to TIMI II flow.3.0 x 30 mm SES stent was deployed at mid LAD - restored TIMI III flow but the patient still had severe hypotension (BP 60/40 mmHg) despite good LAD flow.Angiogram was done again - Lcx and DG1 showed abrupt vessel closure (the rota was done only at LAD!), diffuse coronary emboli after atherectomy was suspected.Sion black wire was crossed to Lcx and restored TIMI III flow, Reverse TAP technique with 2.75x9 mm SES in Lcx and 3.5 x 15 mm SES in LAD were deployed.DG1 was rescued after that. Final angiogram showed TIMI III flow in all vessel, IVUS showed good stent apposition, no egde dissection with some stent expansion in distal LM and Lcx.Patient was safely discharged 3 days later with full neurologic recovery.
rota 1.5 burr.mov
arrest after rota, No reflow and abrupt Lcx:DG closure.mov
Stent Lcx:LM:LAD, reverse tap, final angiogram.mov
Case Summary
When the procedure didn’t go according to the plan, keep calm and rescue the patient first. Plan B,C should be keep in mind.No-reflow phenomenon accompanied with abrupt vessel closure after rotational atherectomy can be occurred at the same time and lead to devastrating situationIn this setting, we suspected diffuse emboli after atherectomy because we advanced the rotablator to LAD but Lcx was abrupt closure.Simple and fast action should be done to safe the patient life