
CASE20220813_001
A challenging Case : PCI to critical ostial LM stenosis with heavy calcification
By ,
Presenter
Viroj Muangsillapasart
Authors
1, 1
Affiliation
, Thailand1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
A challenging Case : PCI to critical ostial LM stenosis with heavy calcification
1, 1
, Thailand1
Clinical Information
Patient initials or Identifier Number
222
Relevant Clinical History and Physical Exam
A 71-year-old female with known underlying HT, DLP, GERD presented with typical chestpain on exertion for 3 months. Her functional class has changed from functional class IIto III. Physical examination was unremarkable
Relevant Test Results Prior to Catheterization
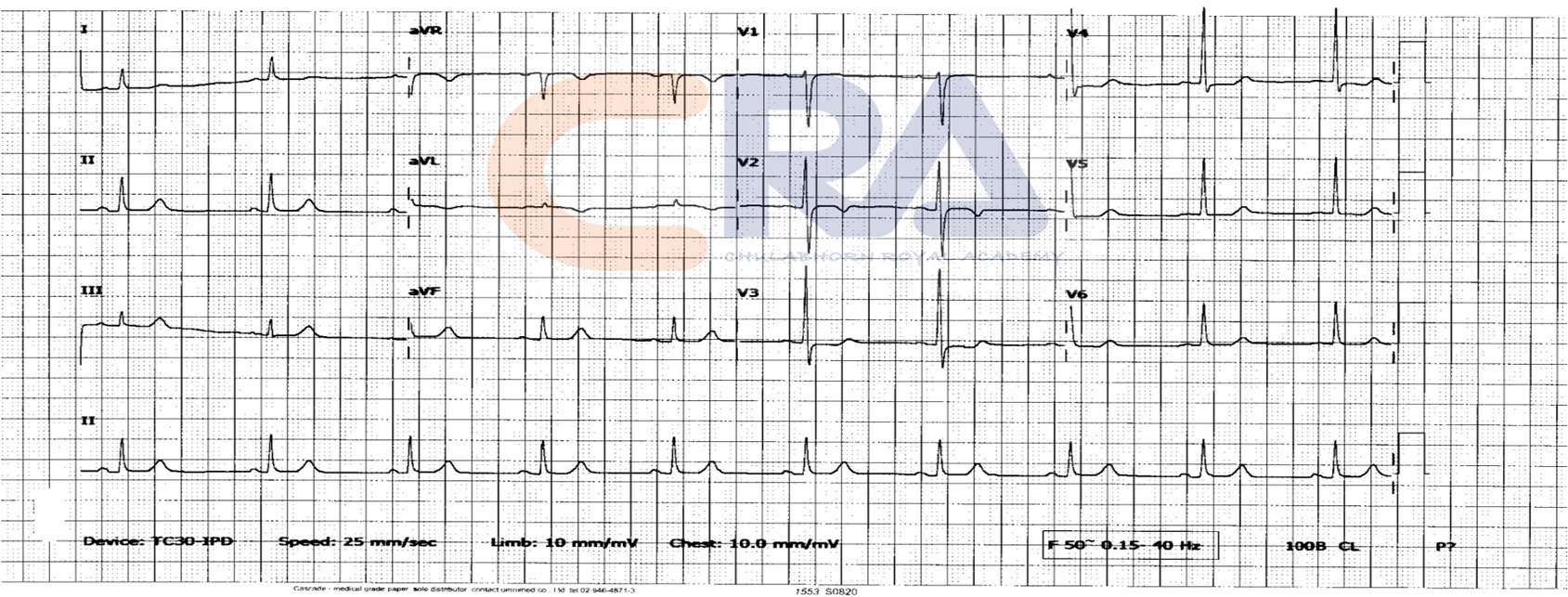
ECG showed TWI in V1-V3 with borderline ST- depression in V4-V6, I,AVL Echocardiogram showed normal LV systolic function with no RWMA, LVEF 65% andno significant valvular disease. Dobutamine stress Echo showed anterior wallhypokinesia.
Relevant Catheterization Findings
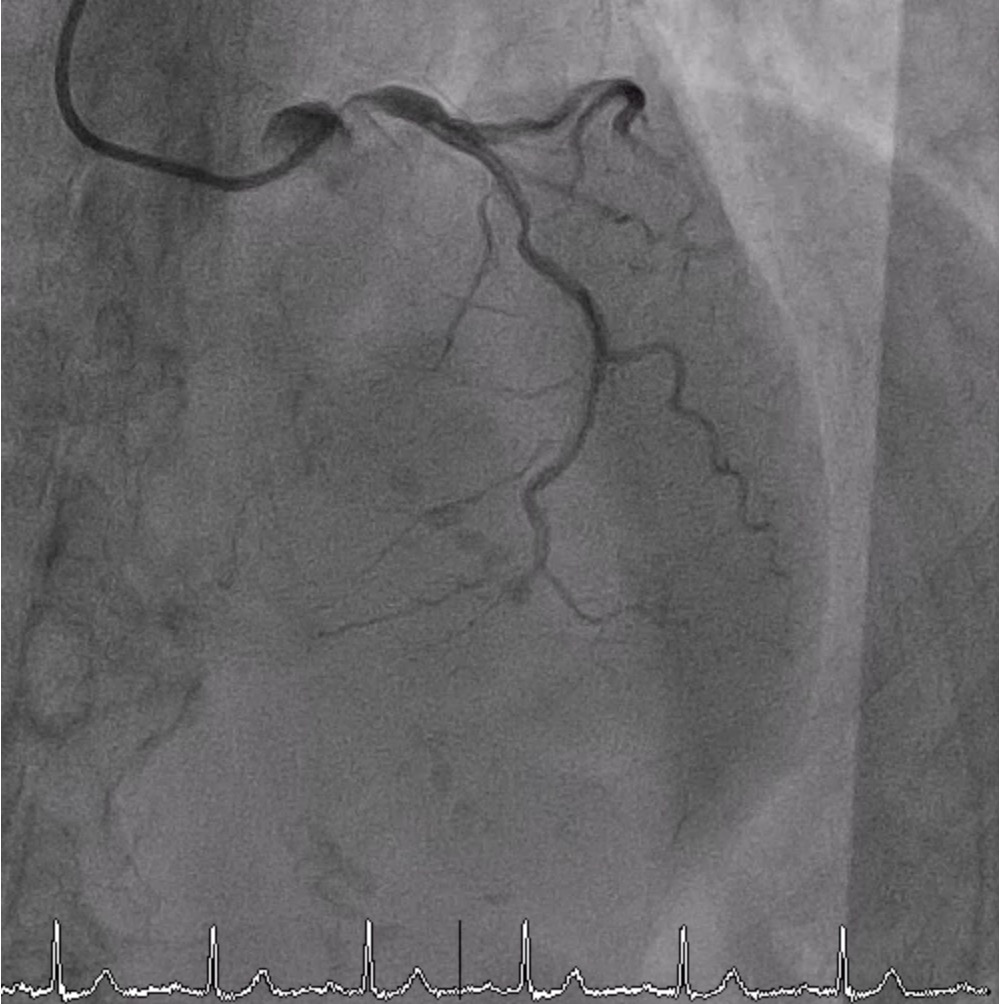
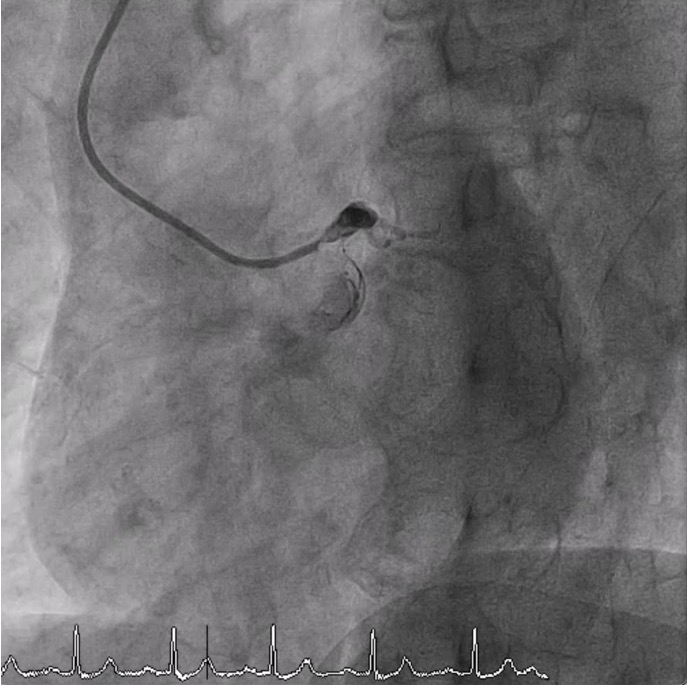
CAG showed severe stenosis 95% at ostial LM (pressure waveform revealed dampingwaveform during engagement of 5 Fr. catheter) with diffused stenosis and heavy calcificationalong LAD. There was significant stenosis of 70% at proximal LCX. RCA was dominant vesselwith mild luminal irregularity.
Interventional Management
Procedural Step
SL 4, 7 Fr was used to engage LCA. Sion Blue passed difficulty to distal LAD because of too much friction. Rotablator 1.5 Burr was performed for eight times. During the procedure, the patient developed severe chest pain.Angiogram showed more severe stenosis at proximal LAD. NC balloon was used for predilatation at proximal LAD then DES 3.5 x 33 mm at LM-proximal LAD was deployed. Because of poor support from guiding catheter, IVUS could not cross mid LAD but revealed significant stent malapposition at distal LM with lumen diameter greater than 5.5 mm . During the procedure, the patient developed bradycardia. HR w as 45-50/min, so atropine w as given then HR increased to 80/min. Angiogram showed coronary perforation Ellis class III. Therefore, prolonged balloon inflation with SC balloon 3.0x15 mm was performed immediately for several times which obtained good outcome. Echo revealed normal LVEF w ith no pericardial effusion. Guidezilla was used due to unable to cross DES to mid LAD. Finally, DES was delivered through guidezilla to be successfully deployed at mid LAD. Final angiogram revealed TIMI flow III at LAD with suspected coronary ectasia at distal LM and clot at mid LAD. However, the patient was agitated and her hemodynamic was stable. Therefore, the decision of the team was ending the procedure and moved the patient to ICU for closed monitoring.
 7-8.mp4
7-8.mp4
11-4.mp4
39-4.mp4
Case Summary
-Severe aorto-ostial lesion – limit contrast flow misleading angiographic severity, PCI planning.