
CASE20220826_007
pLCx CTO and tortuous pLAD. Rotational atherectomy and LM bifucation stenting with provisional stenting to LAD/D1 bifurcation
By
Presenter
Jonathan Xinguo Fang
Authors
1
Affiliation
, Hong Kong, China1
High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention
pLCx CTO and tortuous pLAD. Rotational atherectomy and LM bifucation stenting with provisional stenting to LAD/D1 bifurcation
1
, Hong Kong, China1
Clinical Information
Patient initials or Identifier Number
B47599402
Relevant Clinical History and Physical Exam
78/M . History of PCI to LCx. Mild AS/AR. HTN, Hyperlipidemia. History of ACS. Previous nuclear medicine stress test showed a small inferoposterior infarct.Presents with CCS II-III angina with progressive worsening and also atypical chest pain. Physical exam normal.
Relevant Test Results Prior to Catheterization
Echo: Concl LVH EF55%. Mild AS/AR AVA 1.7cm^2 PG 20/12mmHg. Mild AR.
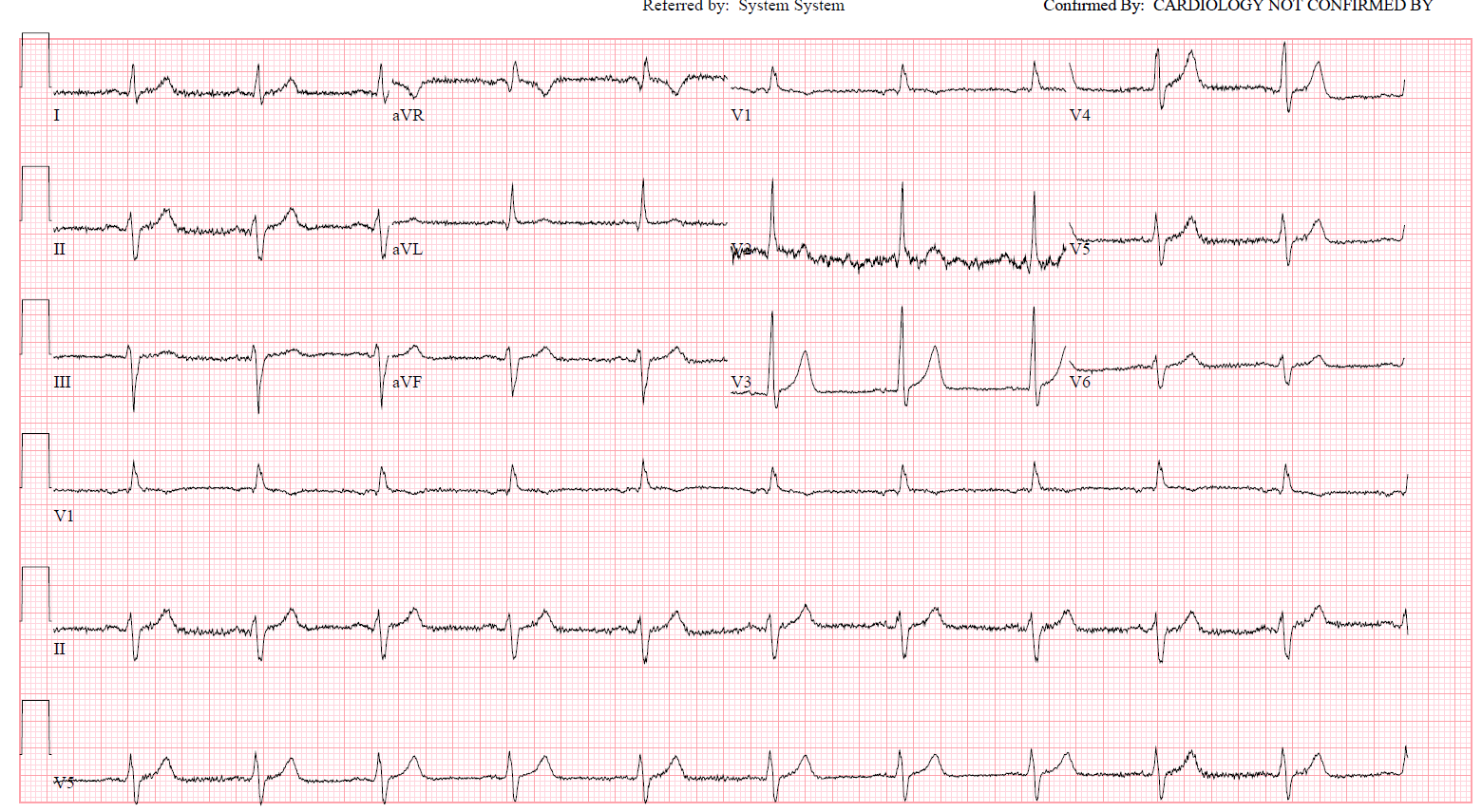
ECG: SR. No Q wave
CXR chest clear
creatinine normal
 MOVIE-0001.mp4
MOVIE-0001.mp4
ECG: SR. No Q wave
CXR chest clear
creatinine normal
Relevant Catheterization Findings
- RCA minor disease – The circumflex in-stent stenosis had progressed to a chronic total occlusion with TIMI 0 flow since the time of the last angiogram– The LAD has a 70 to 80% mid stenosis seen best in the cranial view. Tortuousity over p-mLAD
MOVIE-0001.mp4
MOVIE-0002.mp4
MOVIE-0003.mp4
MOVIE-0004.mp4
MOVIE-0005.mp4
MOVIE-0006.mp4
MOVIE-0007.mp4
MOVIE-0008.mp4
Interventional Management
Procedural Step
PCI to LCx
Noted chest pain, ECG showed V1-V3 STE and diagonal pinched. Rewired over sasuke with pilot 50 and stented with 2.50x15 DES with minimal-protrusion into LAD. postdilation followed by KBI with 2.5 balloon in D and 3.0 balloon in LAD. Nitroglycerin given and chest pain resolved. Subsequent ECG showed slight TWI V1-V3.
MOVIE-0009.mp4
MOVIE-0011.mp4
MOVIE-0019.mp4
MOVIE-0023.mp4
MOVIE-0032.mp4
MOVIE-0036.mp4
MOVIE-0044.mp4
MOVIE-0045.mp4
MOVIE-0048.mp4
MOVIE-0052.mp4
MOVIE-0059.mp4
MOVIE-0062.mp4
MOVIE-0067.mp4
MOVIE-0068.mp4
MOVIE-0076.mp4
MOVIE-0081.mp4
MOVIE-0088.mp4
MOVIE-0090.mp4
MOVIE-0101.mp4
MOVIE-0102.mp4
MOVIE-0112.mp4
MOVIE-0114.mp4
MOVIE-0116.mp4
MOVIE-0123.mp4
MOVIE-0126.mp4
MOVIE-0147.mp4
MOVIE-0151.mp4
MOVIE-0152.mp4
MOVIE-0153.mp4
MOVIE-0004.mp4
RRA 7.5 Fr sheathless. did not give enough support. switched to 8Fr Femoral
LCx ISR STO/CTO crossed with pilot 50. Balloon uncrossable with 1.0. Rotatation atherectomy 1.5 bur 200,000rbpm. IVUS: Severe Ca++. pLCx remained unexpandable with high pressure NC. 3.5 shockwave lithotripsy to pLCx followed by NC and scoring balloon. ostial-pLCx stented followed by high pressure NC optimized with IVUS. 25x38, 3.5x33.
Staged PCI to LAD. 8Fr French sheath. 7Fr EBU 3.5. Rotational atherectomy to LAD 1.5burr 175,000 RPM, patient developed bradycardia despite aminothylline. RFV access wtih temporary pacing wire inserted. predilate with NC 2.5, 3.0 balloons, stent with 3.0x38, 3.0x33 DES to LAD and LM-LAD with 3.5x15 DES. LCx recrossed and stent strut dilated and KBI with 3.5 NC in LAD and 3.0 NC in LCx, followed by POT with NC 4.0 in LM.
Noted chest pain, ECG showed V1-V3 STE and diagonal pinched. Rewired over sasuke with pilot 50 and stented with 2.50x15 DES with minimal-protrusion into LAD. postdilation followed by KBI with 2.5 balloon in D and 3.0 balloon in LAD. Nitroglycerin given and chest pain resolved. Subsequent ECG showed slight TWI V1-V3.
Case Summary
Successful PCI to LCx STO and tortuous LAD , both heavily calcified. s/p rotational atherectomy and completion of 2 step LM-LAD-LCx bifurcation.
Bradycardia during atherectomy needs management with temp pacing even with aminothylline given
Side branch strategy may require KBI or stenting.
Chest pain and ECG change can occur after rotational atherectomy due to distal embolisation even if all side-branches are preserved and TIMI 3 flow to distal vessels are seen.