
CASE20220826_010
How to Deal With In-Stent CTO: More Approach in a Case
By ,
Presenter
Ngo Quang Tung
Authors
1, 1
Affiliation
, Vietnam1
Complex PCI - Chronic Total Occlusion
How to Deal With In-Stent CTO: More Approach in a Case
1, 1
, Vietnam1
Clinical Information
Patient initials or Identifier Number
P.T.V
Relevant Clinical History and Physical Exam
70 y/o female patient.History: HypertensionStent LAD, LCX and RCA 3 year ago (2019)Failed PCI in-stent CTO RCA at localhospital 1 month before admitting our hospital.Clinical presentation:Chest anginaShortness of breath when exertionVitals: BP: 110/70 mmHg; HR: 63beats/min; RR: 19/minPhysical examination normal
Relevant Test Results Prior to Catheterization
| Hb (11 - 16.5 g/dL) | PLT (150 - 450G/l) | Creatinin (44 - 110 μmol/l) | TnT hs (≤ 14 ng/l) | GOT/GPT (< 40 U/L) | Glucose (3.9 - 6.4 mmol/l) |
| 12.6 g/dL | 245 G/L | 67 μmol/l | 4.57 ng/l | 34.9/34.7 U/L | 6.3 mmol/l |
Relevant Catheterization Findings
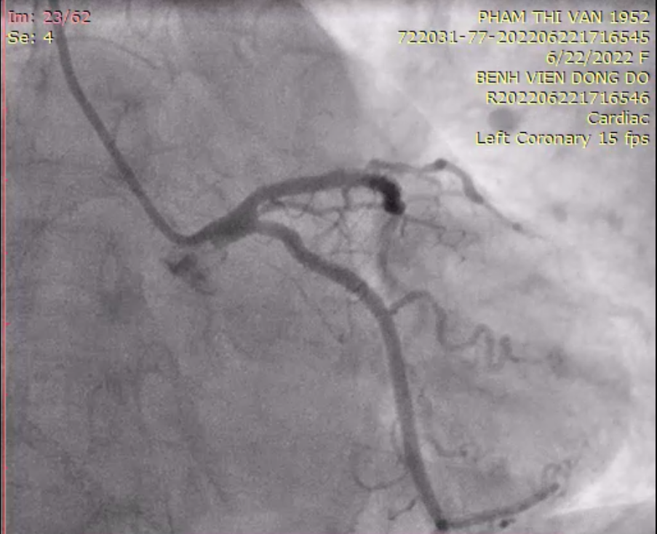
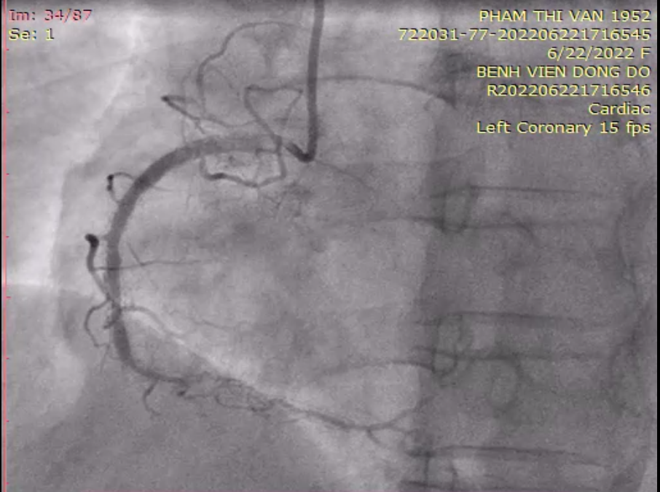
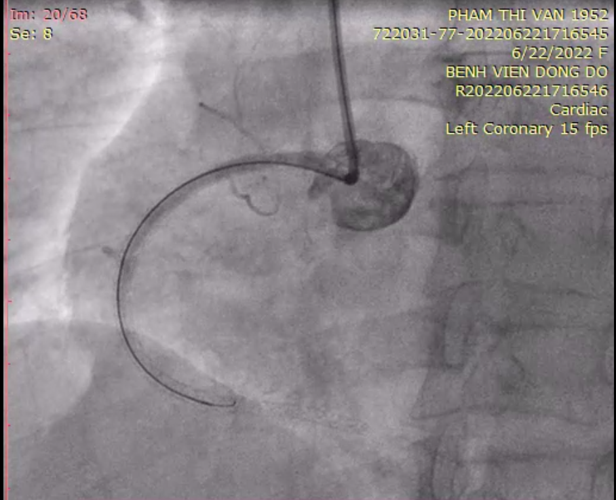
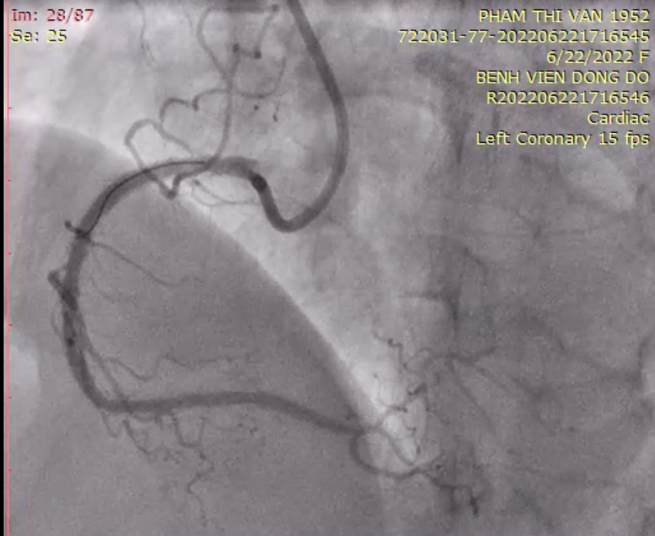
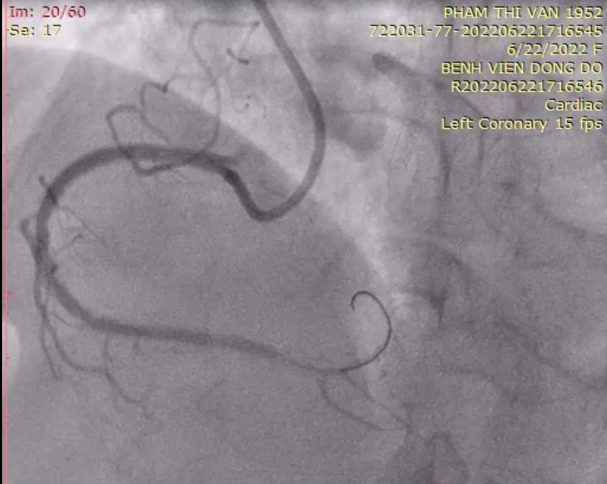
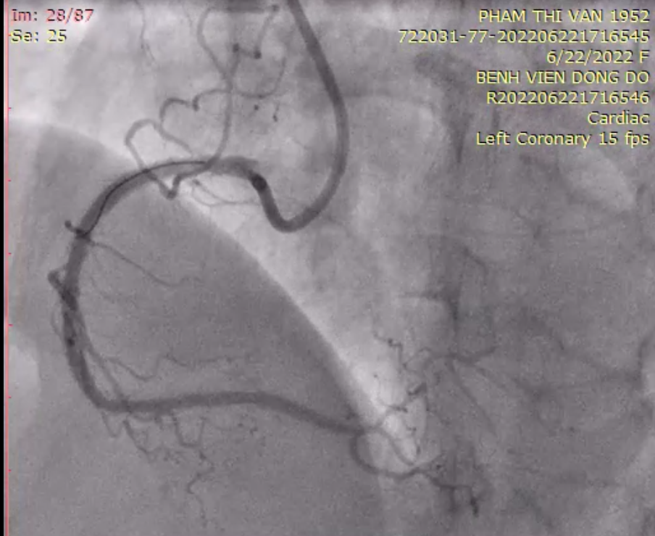
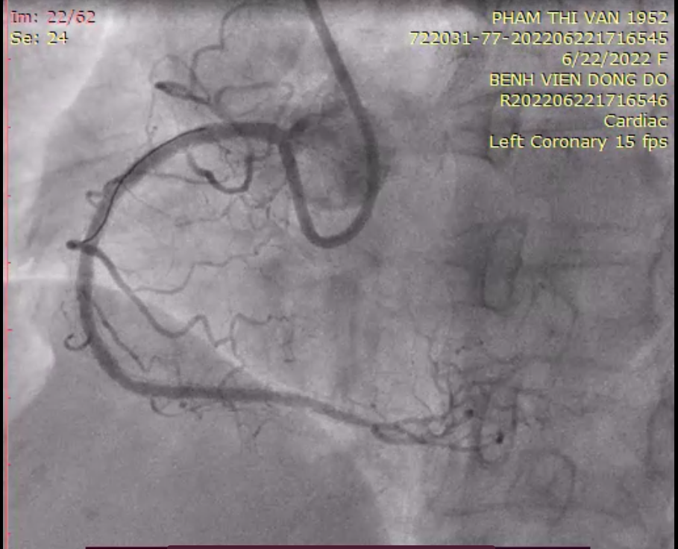
Proximal to distal LCx stent andproximal to mid-segment of LAD stent are still good, TIMI 3 flow with mild atherosclerosis in the stent.About 70% stenosis in mid-segmentof RCA stent, distal CTO of RCA stent with autologous collateral circulationand partial collateral circulation from LAD, LCX branches. The distal segmentafter CTO RCA stent site is relatively small in size.
 LAD, LCX angiography video.mp4
LAD, LCX angiography video.mp4
RCA angiography video.mp4
Interventional Management
Procedural Step
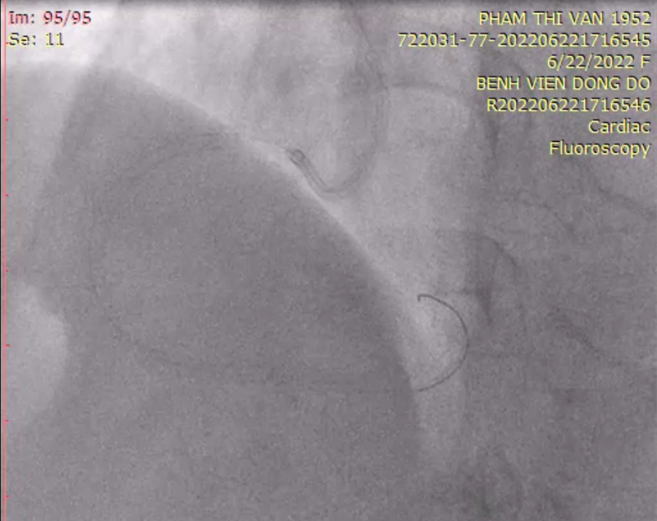
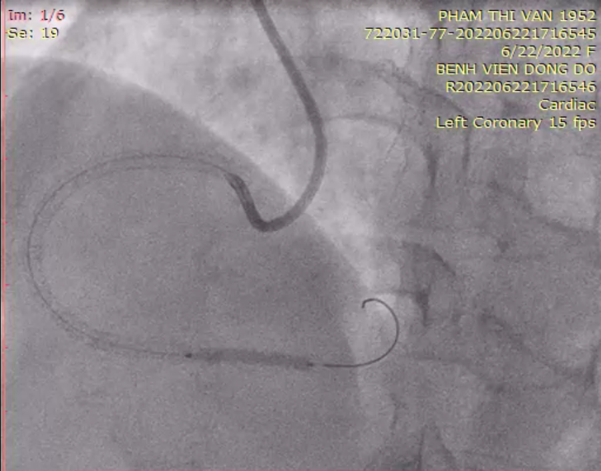
Proximal todistal LCx stent and proximal to mid-segment of LAD stent are still good, TIMI3 flow with mild atherosclerosis in the stent. About 70% stenosis in mid-segment of RCA stent, distal CTO of RCA stentwith autologous collateral circulation and partial collateral circulation fromLAD, LCX branches. The distal segment after CTO RCA stent site is relativelysmall in size. Radial access, 6F Introducer , Guiding JR4, 6 French and Guide wire: Runthrough→ Gaia Second→Fielder XT 0,014 inch. Microcatheter: Caravel 135 centimeter. We have succeeded in advancing the wireand microcatheter through the lesion and into the true lumen of distal vessel. But we failed when we tried to advance a small NC balloon the lesion: Hawk1.5 x 15 mm. Change from JR4 to AL 0.75, 6 French and succeed in advancingguidewire and balloon through the lesion. Predilatation in distal RCAstent with Hawk 1.5x15 mm NC balloon Then we use a bigger balloon:Hawk 2.5x15 mm NC balloon. After pre-dilating, we assessthat there is no landing zone in the distal segment sufficient for stenting,the distal segment size is small, we are concerned about the risk of distaldissection and this is stentnosis lesion. We decided to only do drug-coatedballoon angioplasty (Dior 2.5 x 20 mm) starting at the distalstent site. We also do angioplasty in the mid-segment of the RCA stentwith an NC balloon: Hawk 3.0 x 15 mm. The final result : TIMI 3 flow, TMP 3 and minimal residual stenosis at RCA.
Try to advance wire through the lesion video.mp4
Change JR4 to AL0,75 and succeed in advancing wire through the lesion video.mp4
DCB in RCA video.mp4
Final Result.mp4
predilatation in RCA.mp4
predilatation in RCA.mp4
after predilatation in RCA video.mp4

angioplasty in mid-segment of RCA VIDEO.mp4
FINAL RESULT - LAO.mp4
Case Summary
In-stent CTO PCI remains a challenging procedure,requiring a combination of many different strategies. Choosing guiding withgood support is an important step in CTO, calcification or tortousious lesionsintervention.Drug-elutingballoons remain a valuable option in cases of restenosis in stents or lesionsof small vessels where additional stenting may not be more beneficial to thepatient.